Today Dr Scott Giacomucci facilitated a session for incoming doctoral students at the University of Pennsylvania School of Social Policy & Practice.
The historical, philosophical, and theoretical connections of social work, Sociometry, and psychodrama were presented. Students then engaged in experiential Sociometry processes to explore shared experiences, fears, hopes, and goals.
The TSM circle of strengths was utilized to concretize the collective strengths of the cohort-as-a-whole and create a container of safety and inspiration for the years ahead as doctoral students.
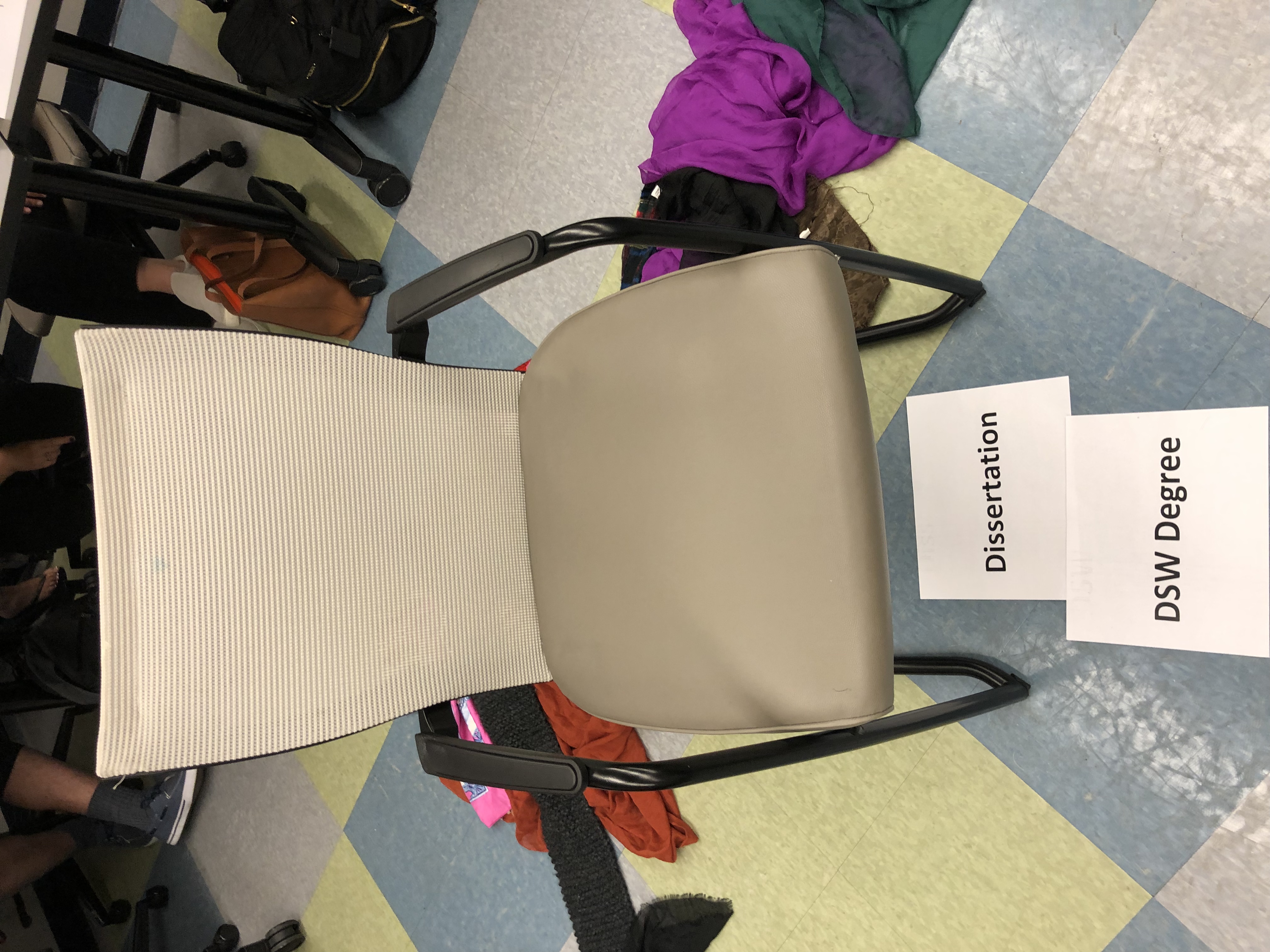
Empty chairs were used to verbalize the positive & negative messages from the dissertation, the DSW degree, future self, and friends/family. Finally, students engaged in a psychodramatic vignette role reversing with themselves as future doctors of clinical social work.
Giacomucci, S. (2019). Psychodramatically Becoming Your “Future Doctor Self”: A DSW First Year Immersion Session. The Clinician, 7(1): 6-7. Access Article Here
Related article here: Giacomucci, S. (2019). Moreno’s Methods in Academia (or the lack of): A Call to Action. Psychodrama Network News. Fall 2019, p. 20. American Society of Group Psychotherapy and Psychodrama.
“It is impossible to
understand addiction without asking what relief the addict finds, or hopes to
find, in the drug or the addictive behavior.” –Dr. Gabor Mate
Among the most common underlying factors
of Substance Use Disorders (SUDS) and other addictive behaviors are unresolved
trauma, neglect and loss. Ignoring these
fundamental issues in treatment results in a focus on symptom control rather
than addressing the actual causes of addiction and relapse.
Addiction and Trauma—a Cyclical Relationship
Addiction and Trauma/loss have a
cyclical relationship, which means they fuel each other. Trauma and loss leave one vulnerable to
developing addictions, and addictions leave one more vulnerable to experiencing
further trauma and loss.
Trauma impacts our ability to
regulate ourselves and our emotions, which is where the addiction comes in to
play a role in helping us self-soothe and numb these emotions. Both addiction
and trauma are characterized by attempts to ‘get out of ourselves’ through
numbing, dissociation, and avoidance. Recent neuroscience research shows that social pain and physical pain look identical in brain scans – any opiate addict
will tell you how well opiates work at numbing both types of pain. These
findings further highlight the intersection between addiction, trauma, and
loss.
Trauma describes any experience that
overwhelms one’s ability to function and cope.
An inclusive definition of trauma might include experiencing or witnessing
violence (relational or collective), abuse (physical, emotional, or sexual),
death or loss, neglect, and abandonment.
Research has demonstrated a strong connection between trauma and many mental health issues—including addictions, depression, and anxiety. Post-Traumatic Stress Disorder (PTSD) symptoms include intrusions, avoidance, hyperarousal, negative thought/mood states and dissociation. These could simply be described as a manifestation of past experiences (feelings, thoughts, images, relationships, physical sensations, defenses, and behaviors) showing up in the present moment.
ACE Study
Research
has shown a strong correlation between adverse childhood experiences (ACEs) of
trauma, neglect and loss, with adult alcoholism and addiction. The ACE study used a simple 10 yes/no
questionnaire inquiring about experiences of trauma, neglect, and family
dysfunction in childhood. For someone reporting four or more ACEs, the results
show a 500 percent increased chance of developing adult alcoholism, and a 1300
percent increased chance of developing an addiction. Higher ACE scores were
correlated with her rates of depression, suicide attempts, and other medical
issues.
4 ACEs =
500% increase in adult alcoholism
4 ACEs = 1300% increase in adult IV drug use
6 ACEs = 4600% increase in adult IV drug use
Trauma Treatment
There are many different approaches to trauma treatment and trauma recovery. While some people find traditional talk therapy to be helpful, other therapy approaches are available and may be more suitable for trauma work. Recent neuroscience research shows that the language/speech parts of the brain are offline when one remembers a traumatic event, which supports the use of or arts-based experiential therapy approaches such as music therapy, art therapy, drama therapy, and psychodrama. In the psychodrama approach, rather than talk about an issue or problem, we can put the situation into action using role-playing techniques and practice new ways of responding. In psychodrama, we could have a dialogue with God, with a deceased loved-one, or even with yourself at a different point in time. Psychodrama allows us to go places in therapy that would be impossible otherwise.
Another highly recommended and effective treatment for trauma is ‘EMDR’ or Eye-Movement Desensitization and Reprocessing. EMDR works by first providing practical tools for dealing with stress, anxiety, and overwhelming feelings. In EMDR, we call these resources; basically, there are about accessing positive memories that can change how we are feeling currently. After the resourcing stage comes the EMDR processing stage during which specific traumatic memories are targeting using EMDR’s protocol. EMDR is incredibly effective for single-incident traumatic events. EMDR and the creative-arts therapies are unique in that you can heal from trauma without having to tell someone every detail of your traumatic experience.
Yoga and meditation
are wonderful resources for trauma and addiction recovery. A recent study found
yoga to be more helpful in reducing PTSD symptoms than any medication that has
ever been researched. Research on meditation supports its effectiveness in
rewiring the brain and strengthening one’s ability to tolerate discomfort,
empathize with others, and find inner peace.
Suggested Books
Bessel van der Kolk, MD – The Body Keeps the Score: Brain, Mind, and Body in the Healing of
Trauma (2015)
Peter A. Levine, PhD – In an Unspoken Voice: How the Body Releases
Trauma and Restores Goodness (2010)
Francine Shapiro, PhD – Getting Past Your Past: Take Control of Your
Life with Self-Help Techniques from EMDR Therapy (2013)
Christine A. Courtois, PhD – It’s Not You, It’s What Happened to You (2014)
Phoenix Center’s Director, Dr Scott Giacomucci, gave a plenary presentation as an honoree at the Global Conference on Addiction Medicine and Behavioral Health in London this morning.
This presentation focused on the cyclical relationship between addiction & trauma and the experiential therapies as a holistic approach to treatment.
The neuroscience evidence is pretty clear. Children who are nurtured, have secure attachment figures, a safe environment, and access to the creative arts develop the capacity for self-regulation, self-soothing, and secure adult relationships.
Adverse childhood experiences often have a lasting impact on one’s development.
Those most likely to thrive are the children who were nurtured.
There also exists a corrective and restorative potential in positive relationships or experiences today. These corrective emotional/relational experiences have the capacity to change and heal the trauma of the past.
This is one of the reasons why psychotherapy is effective – it provides an experience of a safe, secure, nurturing relationship.
Post-Traumatic Stress is simply the past emerging in the present.
Feelings, images, physical sensations, and thoughts from the time of the trauma resurface in the present moment when we are faced with a reminder of the event.
This is really just our bodies & psyches trying to protect us – but it causes lots of problems and impacts our functioning in the world.
Healing from trauma isn’t so much about telling the story of the past as it is about renegotiating how the experience lives with us today. Feelings need to be expressed, sensations experienced, beliefs revisited, and internalized roles transformed.
Treatment providers that don’t address the trauma underlying addictions are only controlling symptoms rather than dealing with the source of the problem.
Being “trauma-informed” is a good start, but not enough. The success rates of addiction treatment are horrendously poor compared to success rates of other conditions. In order to improve treatment quality, the addiction treatment field needs competently trained trauma treatment specialists.
Visit www.PhoenixTraumaCenter.com to learn more about our clinical work, training events, and consultation services for your agency.
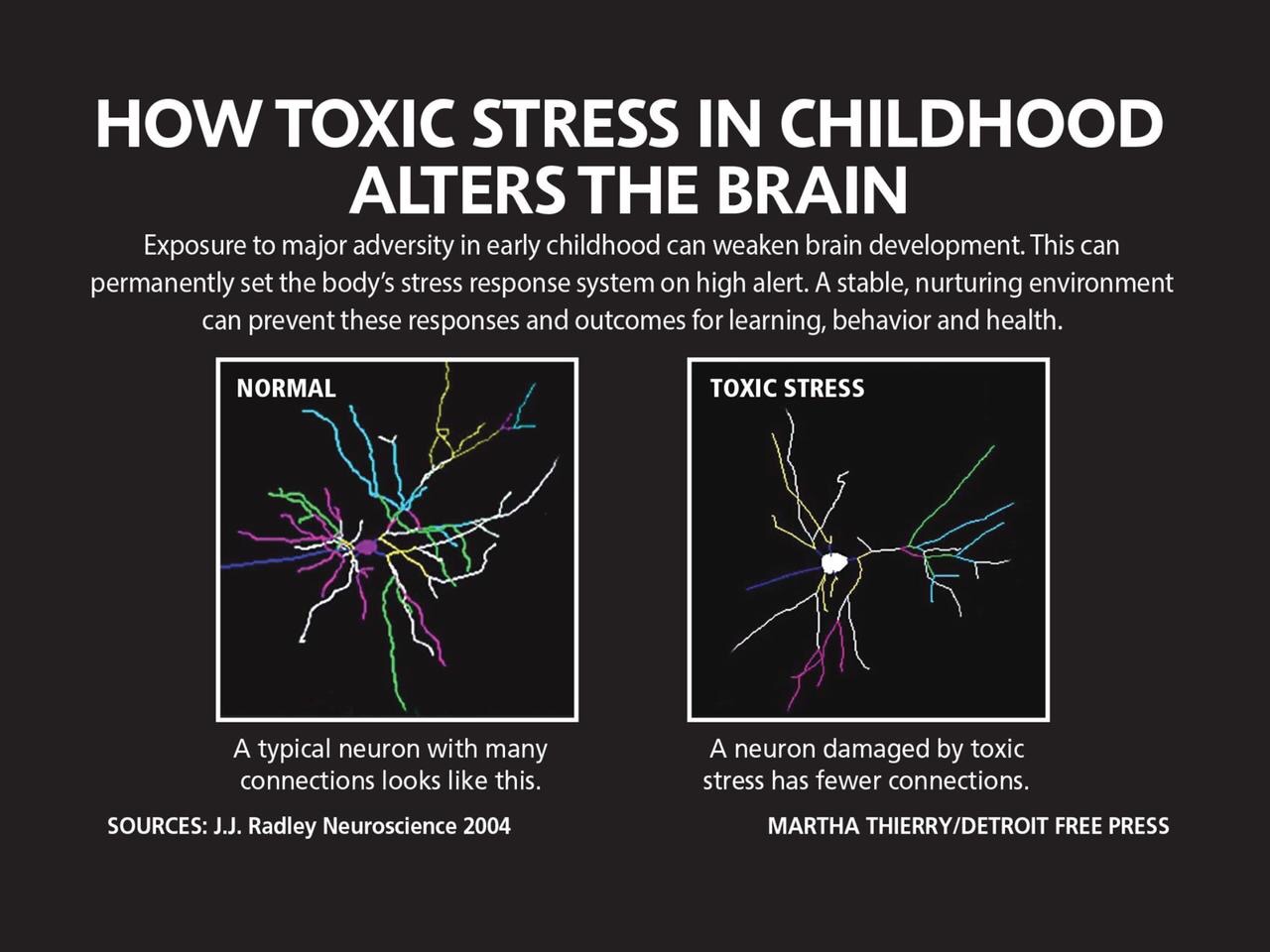
Prolonged and extreme stress (including post-traumatic stress) significantly impacts brain development, especially for children.
The image below on the left shows a typical integrated/connected neuron from a child in a safe nurturing environment, next to an image of a neuron much less connected/integrated from a child who experienced prolonged stress. This type of stress creates fragmentation and dissociation biologically, psychologically, and socially.
Our environment impacts brain development in a very real and lasting way. Cultivating safety is an essential component of healing from post traumatic stress.
We are proud to announce our recognition by the International Society of Experiential Professionals as an Experientially Certified Organization (ECO). We are one of the first organizations in the world to be awarded this credential!
Our commitment to providing experiential therapy services and experiential therapy education/training remains in the forefront of our vision as we expand and grow.
A new publication by Dr Scott Giacomucci – Trauma Survivor’s Inner Role Atom: A Clinical Map for Posttraumatic Growth
The Journal of Psychodrama, Sociometry, and Group Psychotherapy.
Abstract:
The treatment of posttraumatic stress disorder and other trauma-related maladies requires psychotherapists to be equipped with a dependable clinical map that can guide them through the difficulties of trauma therapy. The Therapeutic Spiral Model—a clinically sophisticated and research-supported adaptation of classical psychodrama that has been used in over 30 countries—comes equipped with a comprehensive clinical map called the Trauma Survivor’s Inner Role Atom (TSIRA), which emphasizes safety, containment, and strengths. The Trauma Survivor’s Inner Role Atom provides a guide to intrapsychic structural change conceptualized in the simplicity of role theory while drawing from continued developments in neuroscience research. It offers a triune map beginning with prescriptive roles to build strengths, connection, accurate observation, containment, and safety. The trauma roles offered by the model’s intrapsychic trauma triangle are explored only after the prescriptive roles have been established, with the clinical functions of each demonstrated. And finally, the transformative roles—the internal manifestation of posttraumatic growth—emerge and are integrated as a completion of the clinical map’s three spirals. The implementation of this inner role atom as a clinical map prevents retraumatization while providing emotional regulation to protagonists and the group, keeping them within their window of tolerance.
Trauma exists upon a continuum or a spectrum.
There are experiences that we often describe as capital “T” Traumas, and other experiences
that we refer to as lower-case “t” traumas. Both can be equally disruptive in
one’s life, especially when experienced over and over again. One of every four
adults, and one of every two children, that experience a traumatic event will develop
PTSD symptoms.
It seems appropriate that PTSD and trauma are
often responded to with denial or dissociation – attempts to defend or protect
one’s self from the vulnerability and reality of surviving a traumatic event. However,
in order to fully recover from trauma and PTSD, one must come to a place of
acceptance of their past. Post-Traumatic Stress Disorder (PTSD) is one of the
most poorly understood mental health disorders. Interestingly, it is also one
of the few diagnoses which asks, “what happened to you?” rather than “what is
wrong with you?”.
What Is
Trauma?
According to Dr. Peter Levine, an expert on
traumatic stress:
“Trauma is a basic
rupture – loss of connection to ourselves, our families, and the world. The loss, although enormous, is difficult to
appreciate because it happens gradually. We adjust to these slight changes,
sometimes without taking notice of them at all…although the source of
tremendous distress and dysfunction, it (trauma) is not an ailment or a
disease, but the by-product of an instinctively instigated, altered state of
consciousness. We enter this altered state let us call it “survival mode”
when we perceive that our lives are being threatened. If we are overwhelmed by
the threat and are unable to successfully defend ourselves, we can become stuck
in survival mode. This highly aroused state is designed solely to enable
short-term defensive actions; but left untreated over time, it begins to form
the symptoms of trauma. These symptoms can invade every aspect of our lives.”
One of the most effective ways to evaluate if
you have been traumatized is to answer these simple questions about a
significant incident: when you remember the incident, is the memory exactly the
same every time? Or, is the memory fragmented or difficult to recall?
If an answer is yes, then the memory is likely
a traumatic one. By no means does one
traumatic memory constitute a diagnosis of PTSD; however, it does indicate that
the traumatic event has been stored in an unprocessed manner and continues to
cause you distress or require the defense of dissociation to avoid fully
accepting what happened.
What is
a PTSD Diagnosis?
The Diagnostic and Statistical Manual of Mental Disorders or DSM5, offers multiple criteria for a PTSD diagnosis.
The first criterion relates to the actual trauma:
Directly experiencing the traumatic event(s)
Witnessing, in person, the event(s) as it occurred to others
Learning that the traumatic event(s) occurred to a close family member or friend
Experiencing repeated or extreme exposure to aversive details of the traumatic event(s); this does not apply to exposure through media such as television, movies, or pictures
The next four criteria for PTSD are outlined in this graphic:
According to Levine, “The symptoms of trauma may be continually present or they may come and go. They may even surface after being hidden for decades. Usually, symptoms do not occur individually, but in clusters grow increasingly complex over time. Unfortunately, they become less and less connected with the original traumatic experience, making it increasingly difficult to trace the symptoms to their cause, and easier to deny the importance of the traumatic event in one’s life. However, if we pay attention to these symptoms, for what they are – internal wake up calls – we can address and begin to heal our trauma.”
Experiencing trauma and/or PTSD is not rare
or uncommon. While many may suggest seeking treatment is a sign of weakness, we
would argue that it is a tremendously courageous act. Though it may not feel
possible at times, many trauma survivors report that they experienced growth
and positive changes after a traumatic experience and/or the treatment of PTSD –
this has been termed Post-Traumatic Growth.
Post-Traumatic Growth is not a new idea, it exists within all legends, myths, and holy books throughout time. The phenomenon of growing after hardship is quite common – nevertheless still remarkable. There are five common domains of post traumatic growth which include a new sense of personal strength, new possibilities, new appreciation of life, stronger emphasis on relationships, and spiritual/religious/existential changes. Even more hopeful, is the fact that around 2/3rds of trauma survivors report experiencing post-traumatic growth, making it more likely statistically than PTSD. After experiencing trauma, you are actually more likely to growth from it than to develop PTSD!
If you or someone you love may be impacted by trauma or post-traumatic stress, reach out to us for help at 610-203-2877